|
2. |
WATER IMMERSION TECHNIQUE IS PAINLESS BECAUSE THE COLON IS NOT ENLOGATED |
WHAT MAKES COLONOSCOPY
PAINFUL?
What makes colonoscopy so painful? As a matter of fact, surgical removal of polyps does not cause pain, because the colonic mucosa does not contain a nerve to feel pain. Actually, the cause of pain during colonoscopy is elongation of the colon. For example, when you eat large amount of food you do not feel pain until you eat more than a comfortable threshold volume. That is, once the intra-stomach-pressure gets high enough, you feel pain. As such, when the luminal wall is pressed with the force of under 1 kgw it does not cause much pain, but when the force exceeds 2 kgw it produces pain.
Å@
 |
Å@
TALKING
POINTS: WHAT MAKES
COLONOSCOPY PAINFUL 2) Just like the stomach, the
elongation of colon can cause pain.
1) There is no pain as
long as you eat a moderate amount, but when you eat more
it can cause terrible stomach pain.
Å@
THE DIFFICULT AND PAINFUL PART IS
THE UNFIXED PART OF THE LARGE INTESTINE: TRANSVERS COLON AND
SIGMOID COLON
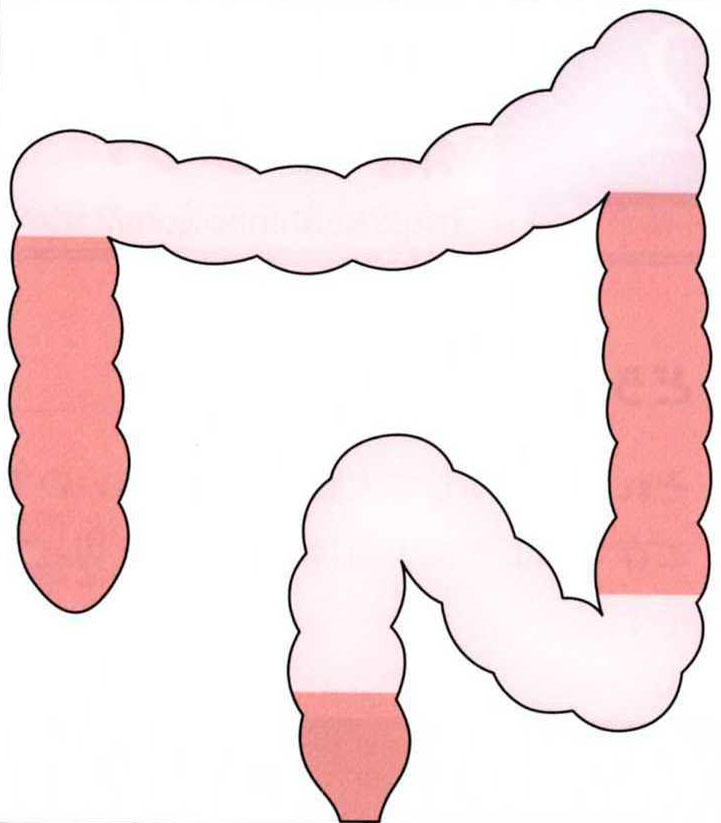
Scope intubation has a reputation for being difficult and painful. In exactly what part is this so? Anatomically, there are two segments of the colon: the fixed part and the unfixed part. The fixed part is the ascending colon, descending colon, and rectum. The unfixed part is the transverse colon and sigmoid colon. The fixed part is simple and easy to scope, and what makes colonoscopy difficult is the unfixed part, the transverse colon and sigmoid colon. When this part is elongated by the scope, pain occurs. The key to success is how to pass this region.
Å@
WHY IS THE INTESTINE
ELONGATED
Forceful pushing easily elongates colon. So can insufflated air.
|
TALKING POINTS: WHY IS THE INTESTINE ELONGATED? 1) Scope pushing. |
Å@
a) PUSHING THE SCOPE ELONGATES THE
COLON.
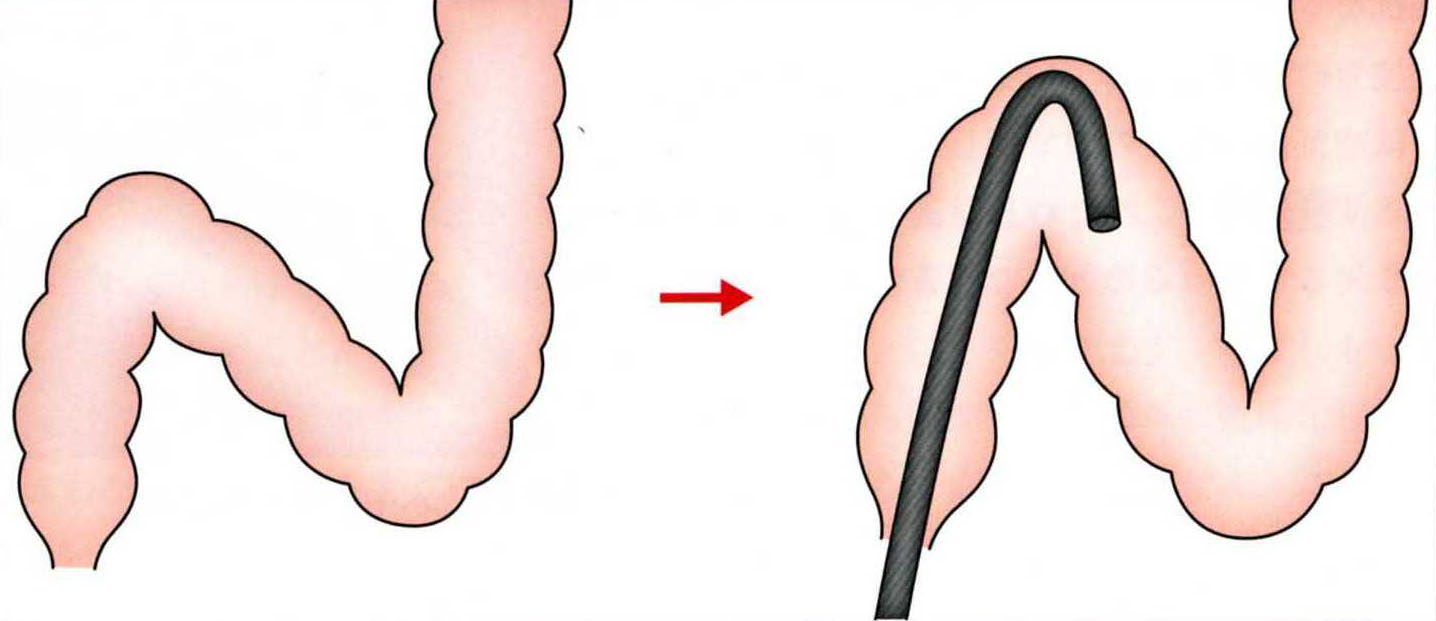
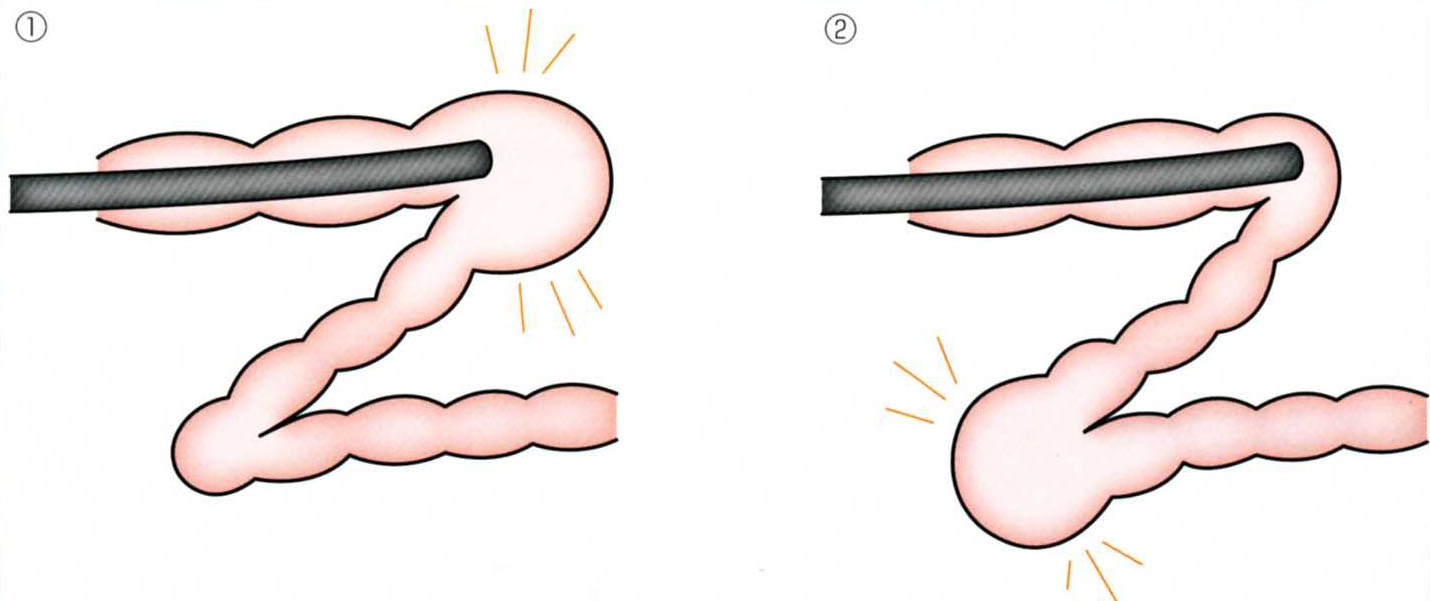
The original shape of sigmoid colon is folded like a deflated accordion and nearly straight. When the scope reaches a certain point in the sigmoid colon, "S-top", where the sigmoid colon is divided into two parts, S-former half and S-latter half, further pushing causes sticking up the colon, making an acute angle. You can tell that the S-top was reached by the paradoxical movement in the vision, that is, the lumen appears to come closer when you pull the scope and appears to back away when you push. If you ignore this movement and keep pushing, the initially escaping view starts moving forward again. The acute angle at the S-top becomes dull with the scope's elasticity and this movement leads to the twist of intestine and loop formation. Therefore, it is very important not to elongate the intestine when pushing the scope.
Å@
Å@
Å@
LUBRICATION AND BUOYANT
FORCE
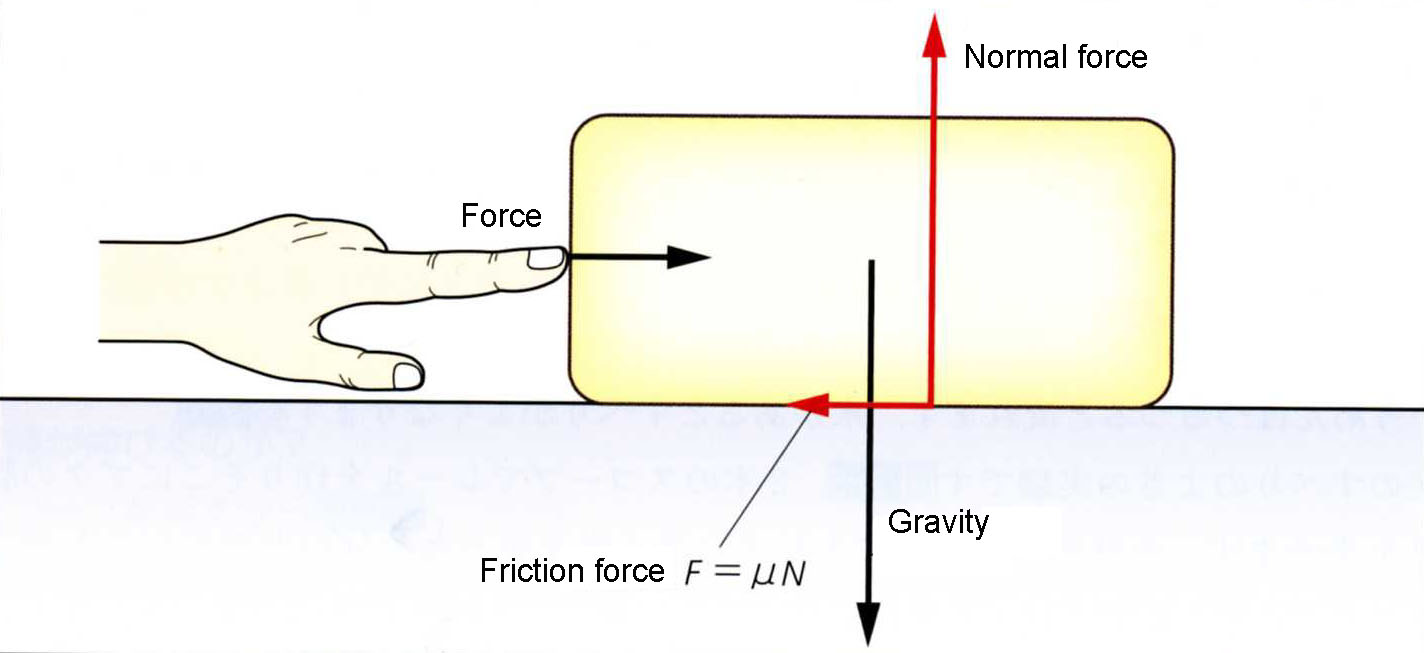
Think about when driving and stepping on your brake pedal on a rainy day. Or when you have slipped and fell on a wet floor. Water works like lubricant.
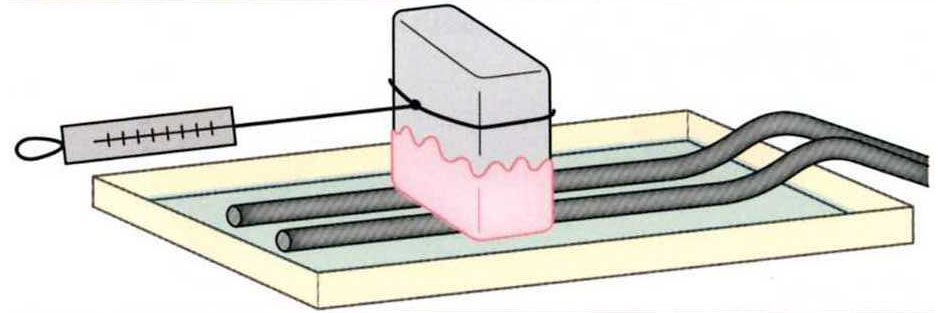
Here is the experiment to show how the scope is lubricated with water. Put a weight covered with pig's gut on a rail of two fiberscopes on a tray. When there is some water in the tray, weight can be pulled with half force. That means when water exists the coefficient of friction becomes half and slipperiness becomes double.
Also, in the water buoyancy forces work. With Water Immersion Technique, the intestinal lumen is filled with water, so the scope will receive buoyant force. Specific gravity of the fiberscope is approximately 2, so the weight of the scope is half in water. Therefore, the force with which the scope pushes against the wall (the normal force) will become half.
With the synergetic effect of lubrication and buoyant forces, the scope can be pushed without much resistance in water. Friction force is equal to the product of the friction coefficient and the normal force (1/2 x 1/2=1/4), which means that with Water Immersion Technique it takes only one fourth of the force that is needed in the air insufflation method to advance the scope. It makes it possible to insert the scope deeper without elongating the intestine.
Å@
Å@
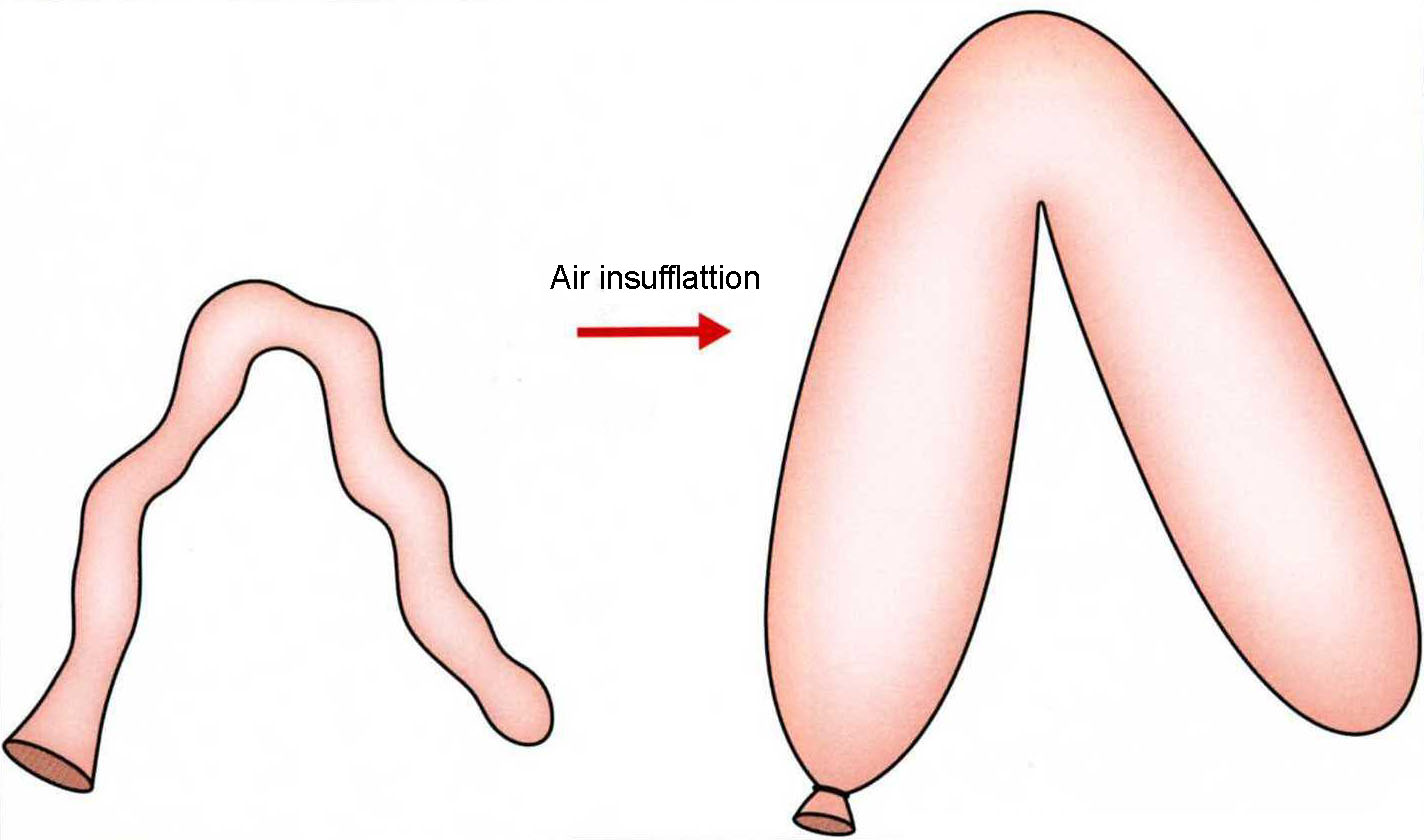
b) THE INTESTINE IS ELONGATED WITH
AIR INSUFFLATION
Mentors have taught practitioners for a long time "do not insufflate air too much" or "make sure to suction air." What is the problem with too much air? The intestine is collapsed like a deflated balloon before air is insufflated. When a great deal of air is insufflated, the intestine gets elongated and bends in the middle. Beginner endoscopists tend to put even more air into the intestine at the bend where they cannot get a good view of the lumen ahead, which makes the bend sharper and it will be even more difficult to tell which direction to advance. But an even worse thing is that it becomes very hard to shorten the intestine when there is great amount of air. A deflated balloon can be easily shortened and straightened, but an inflated balloon is hardly straightened because of its resilience. It is called "shortening-resistant." On the other hand, with Water Immersion Technique the intestine does not have shortening-resistance since no air is used and the intestine stays collapsed.
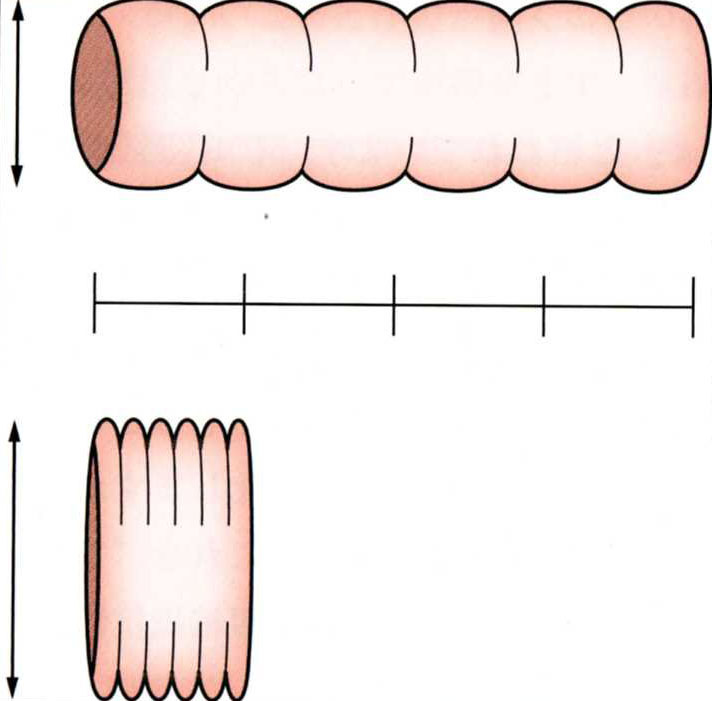
Then why does the intestine not have shortening-resistance when collapsed? When the intestine is shortened and straightened it is folded like and accordion, but the mucosa of the intestine does not stretch beyond a certain point, like skin. As the intestine is shortened, the air loses space and instead pushes the wall and inflates the intestine. Mathematically, if the intestine shortened to one fourth its diameter it becomes twice what it was. In other words, if the intestine cannot become as big as that, shortening is impossible. Therefore, deflating enough air and collapsing the intestine before shortening is important. Conversely, only by deflating air the intestine is shortened and straightened. The intestine is nearly straight in its original state before air insufflation.
Å@
Å@
Å@
|
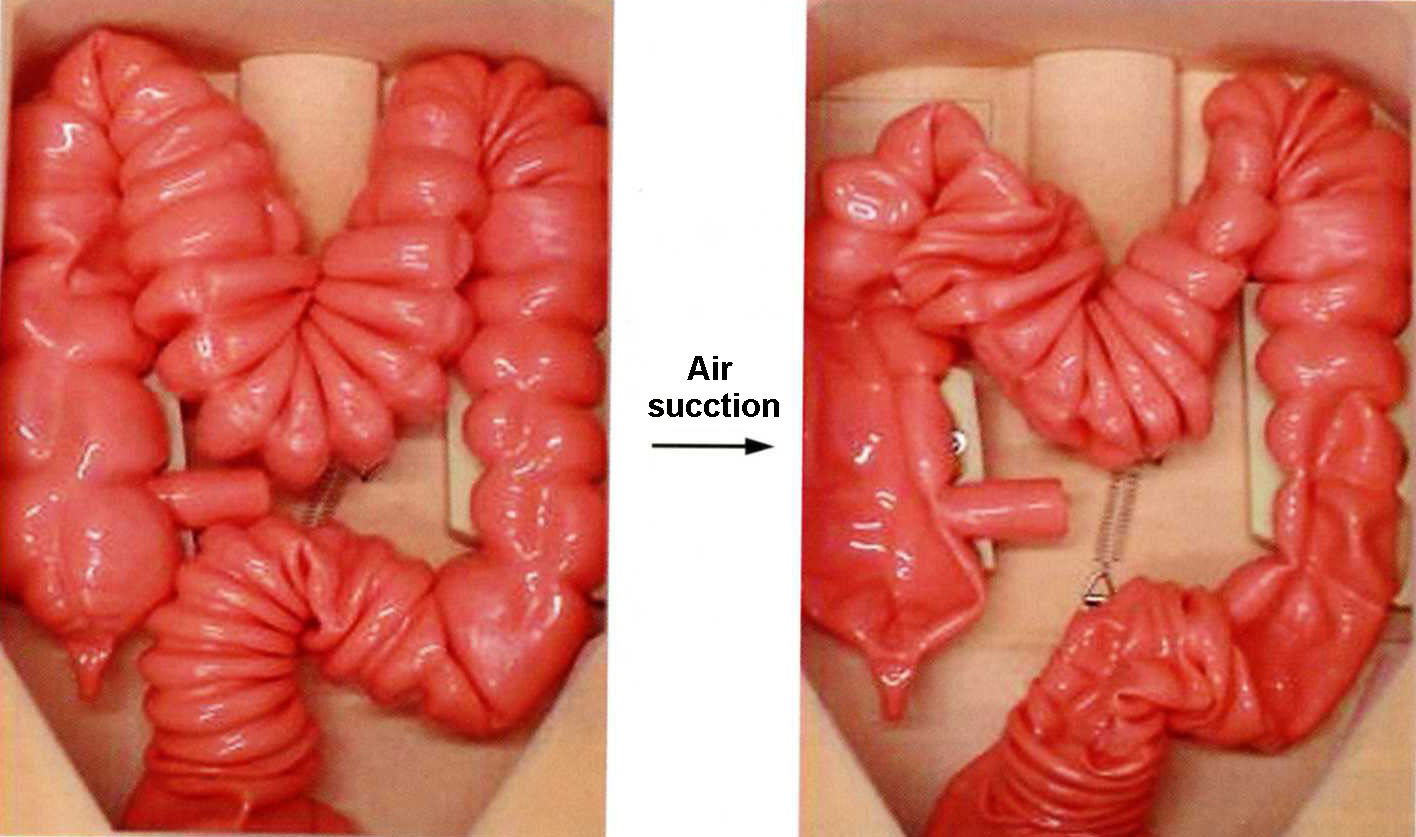
[MOVIE 2-1] This Colon Model was originally created as a practice instrument for air insufflation technique. With air in it, the colon will return to its original position against an attempt of shortening at the mid-transvers colon. It's the same when pressing at S-top. The air-insufflated colon behaves like this model. That means that the colon is "shortening-resistant" when it is filled with air. |
Å@
|
[MOVIE 2-2] When air is suctioned with a vacuum, the intestine is collapsed and it represents a model of Water Immersion Technique. At this time, even when pulling up mid-transverse colon or pushing down S-top, the intestine will not return to the original position. The collapsed colon is not "shortening-resistant". |
WHY DOES WATER IMMERSION TECHNIQUE
NEED ONLY SMALL ANOUNT OF WATER?
Why does Water Immersion Technique require only small amount of water? Beginners tend to insufflate water at the bend of S-top, but the air diffuses quickly and more air makes a sharper bend. Unlike air, water stays for some time and gradually falls down to the lower part of the intestine, that is SD, and that makes insertion easier. Air should not be insufflated at the sharp bend, however, though water is not a problem here. That helps beginners find the way to advance. The amount of water needed for a patient is about 100~200cc and with this small amount of water, the intestine will stay collapsed.
[Inset 2-11 NOT MUCH WATER IS REQUIRED] |
||||
Å@
WHY IS WATER IMMERSION TECHNIQUE
PAINLESS?
1) No push, no elongation of the colon.
2) A little water will not elongate the intestine.
Å@
In conclusion, with Water Immersion Technique, water lubricates the scope and more smooth insertion will not elongate the colon. In addition, water used in this technique is a small amount, such that the intestine will not be elongated. Also, shortening the intestine before it is elongated is possible. That is why Water Immersion Technique is painless.