|
8. |
HOW TO HOLD THE SCOPE-PUT THE SCOPE HEAD ON THE PALM |
FLOW OF THE TRAINING
Before starting the colon model training, learn the basic maneuver with the scope on a bed. The key here is to master using the angle and rotation effectively and smoothly and learning the coordinated movement for releasing the loop. It is a very important step because beginners often fail to traverse the fold for insufficient angulation and rotation.
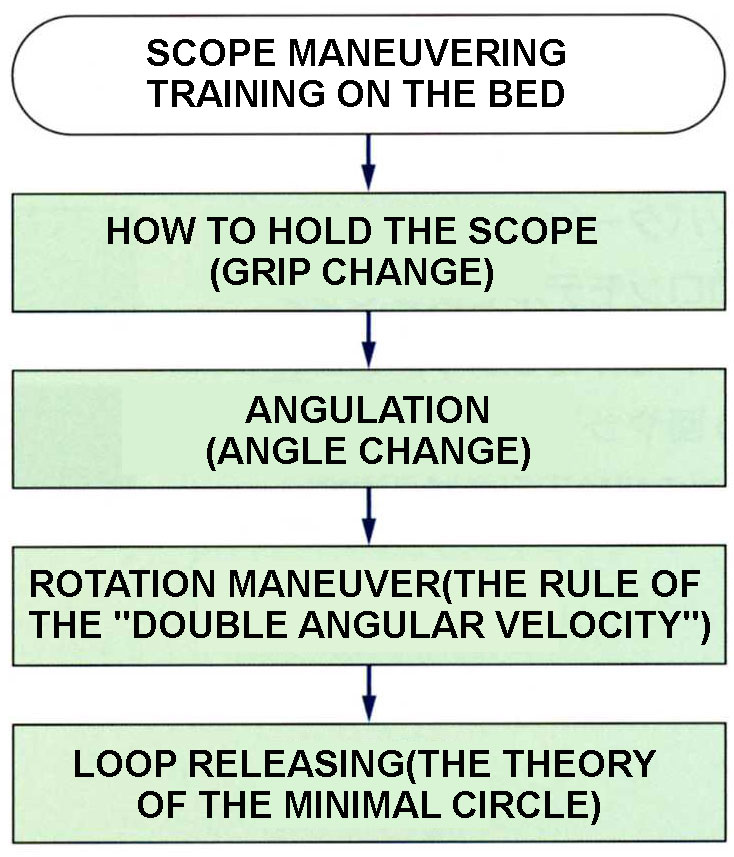
CHART 8-1
Å@
HOW TO HOLD THE
SCOPE
Grab the scope first. Traditionally the scope was held with its head upright (Chart 8-2). This is because when the fiber scope was an optical device it needed to stand upright for the endoscopist to look into the lens, in other words, it is just a remnant from the days of optic scopes. There is no scientific basis for holding the scope upright. With the electronic scope less bending is better so the scope head should be put horizontally.
First face the left palm upward and put the scope on it as if putting it on a tray (Chart 8-3). Holding the scope this way makes it possible to decrease the bending of the scope to the minimum and to rotate the scope with the left hand.
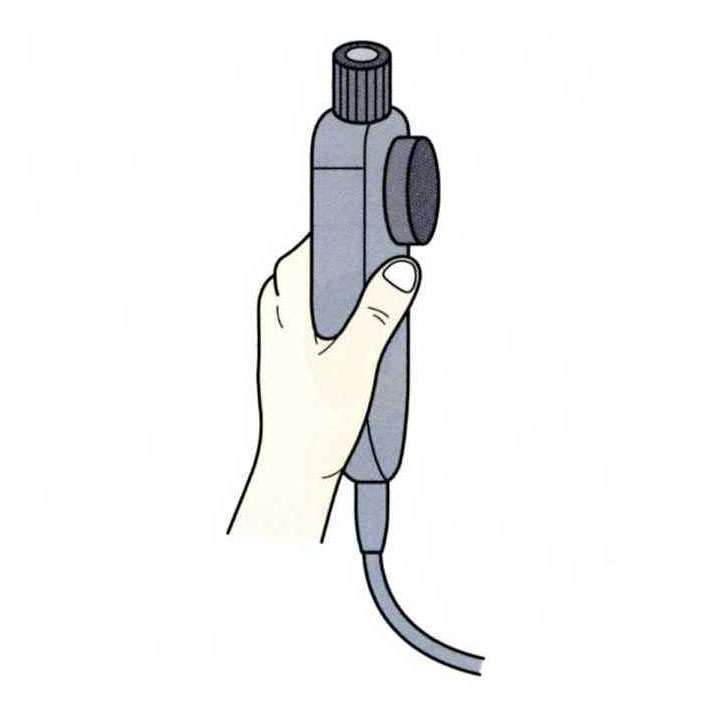
CHART8-2 THE OPTIC SCOPE WAS HELD UPRIGHT. THE SCOPE USED TO BE HELD UPRIGHT FOR THE ENDOSCOPIST TO SEE THROUGH THE LENSE AT THE TOP. |
Å@
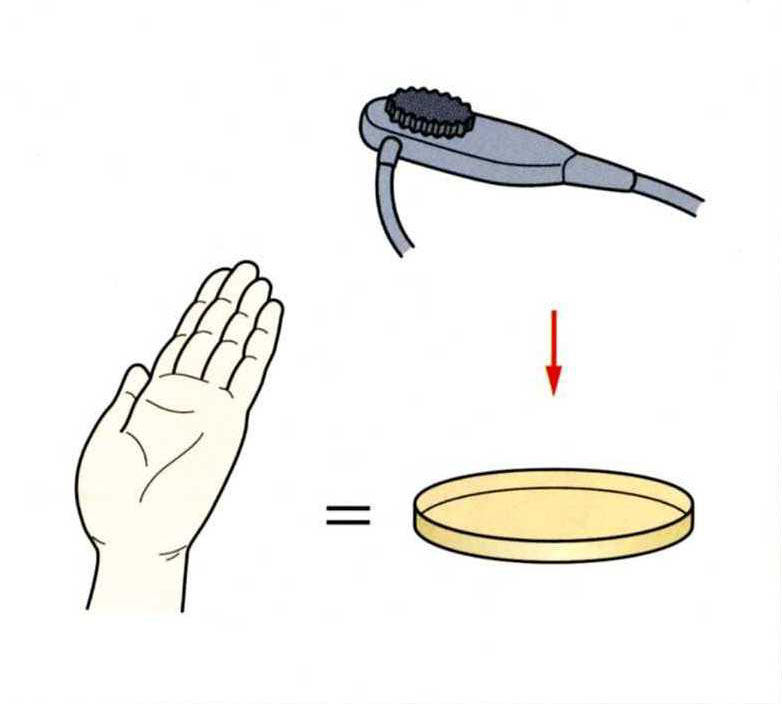
CHART8-3 ELECTRONIC SCOPE SHOULD BE HELD HORIZONTALLY. PLACE THE SCOPE ON THE PALM AS IF IT IS ON A TRAY. |
Å@
The positional relationship between the connector cable, which connects the scope and the video device, and the right arm is shown in Chart 8-4. The left picture is the good example, with the connector cable under the right arm. In the Singular Method left and right angulations are frequently used. With this holding even a small hand can perform left and right angles with a thumb.
The correct left hand position is shown in Chart 8-5.
1) Hold the scope horizontally on the palm so that the angulation knobs are always facing upward.
2) The left hand should be a little away from the scope head so that the angulation knob is used with keeping the thumb straight.
3) Do not hold the scope too tightly since the base of the thumb has to move freely when it shifts from the up-and-down (U/D) angulation knob to the left-and-right (L/R) angulation knob.
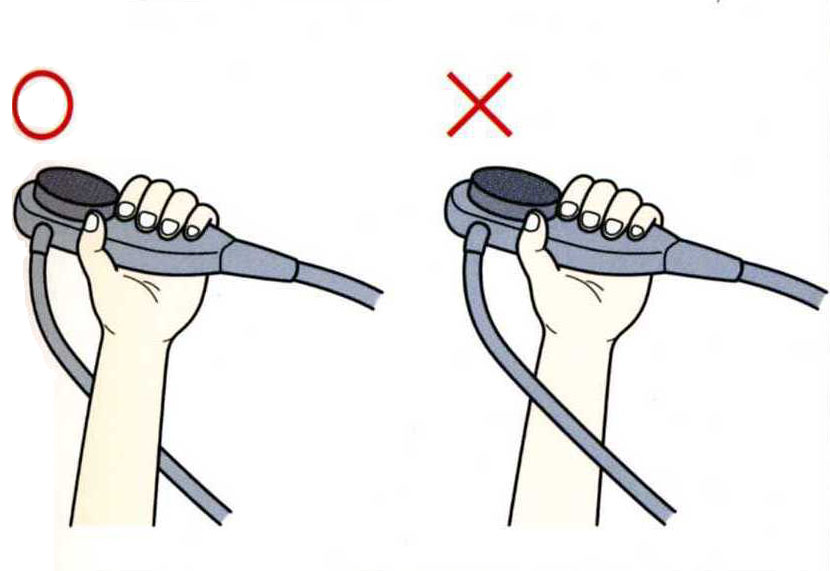
CHART 8-4 DROOP THE CONNECTOR CABLE CONNECTOR CABLE SHOULD BE DROOPED UNDER THE LEFT ARM. |
Å@
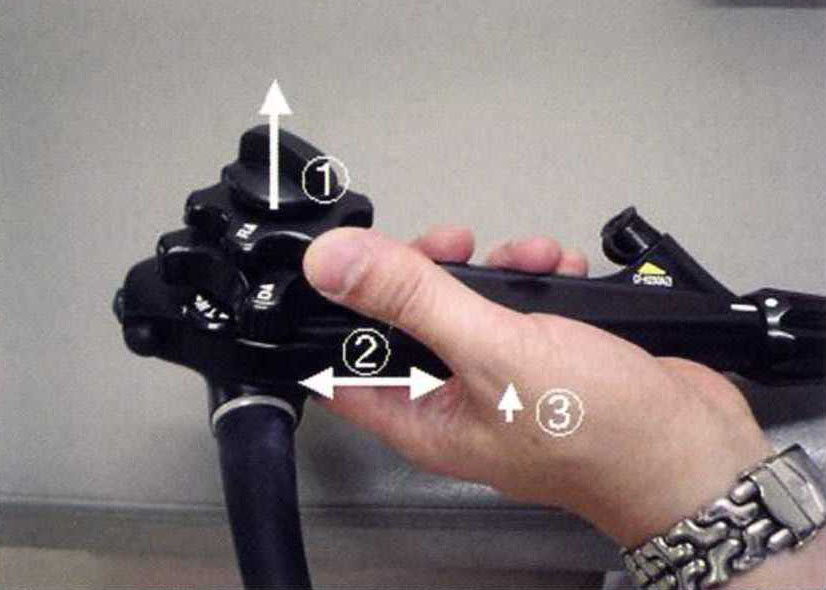
CHART 8-5 RECOMMENDED LEFT HAND POSITION 1) A PALM AND ANGULAITON KNOBS FACING UPWARD. 2) KEEP THE THUMB STRAIGHT AND HOLD SOME DISTANCE FROM THE HEAD OF THE SCOPE. 3) SHIFT THE THUMB WHEN USING THE L/R ANGULATION KNOB. |
Å@
Experienced automobile drivers keep some distance from the driving wheel and hold it softly. Likewise, the right hand holding the scope shaft should not be too close to the anus of the patient and it should not grip the scope too tightly. Thereby maneuver is more effortless and the right hand can feel "the touch" more clearly to sense the information of the scope in the intestine, such as bending or bowing.
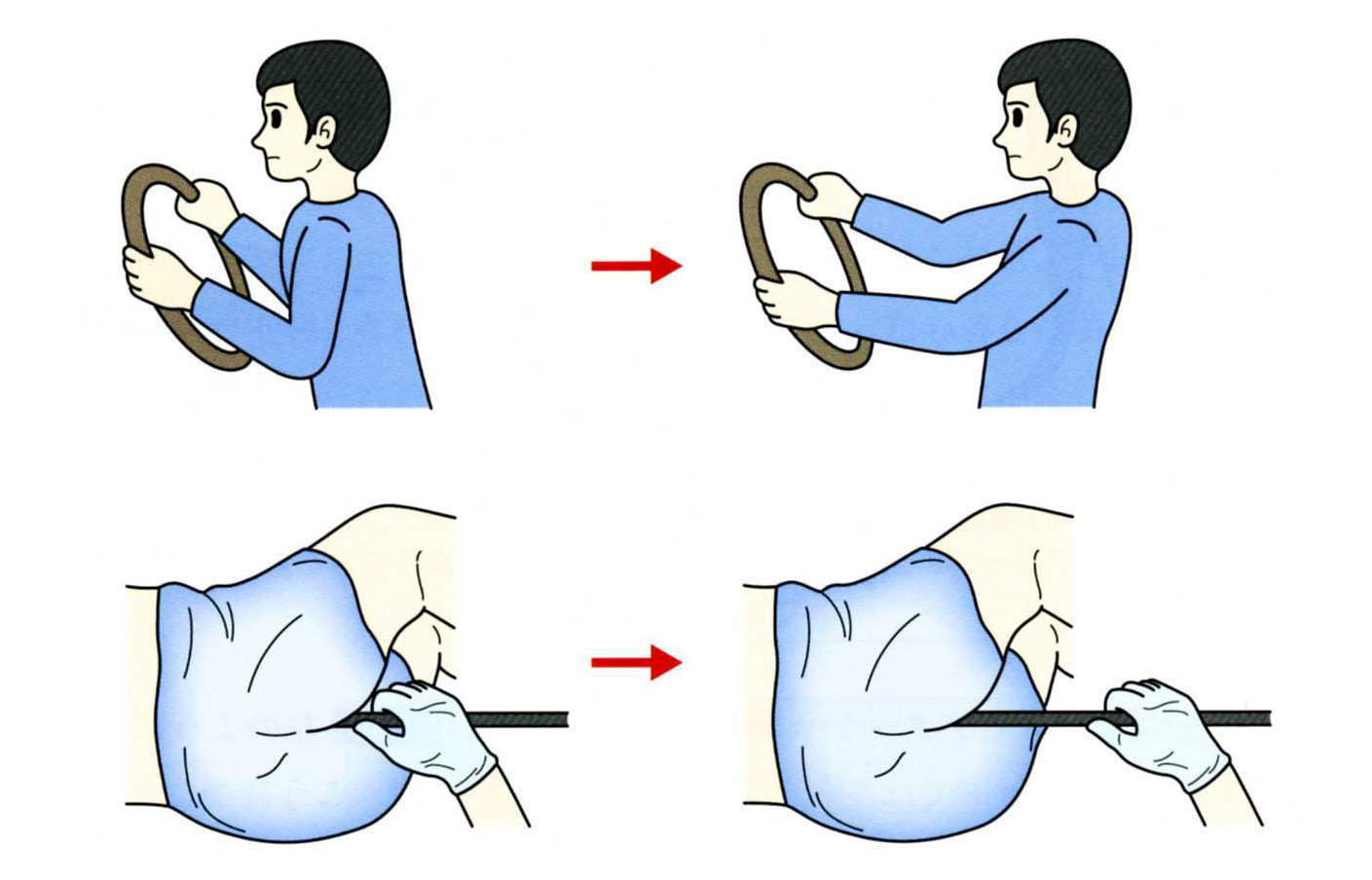
Å@ CHART 8-6 THE DESIRABLE RIGHT HAND POSITION EXPERTS KEEP THE RIGHT DISTANCE AND DO NOT USE UNNECCESARY FORCE. |
Å@
Å@
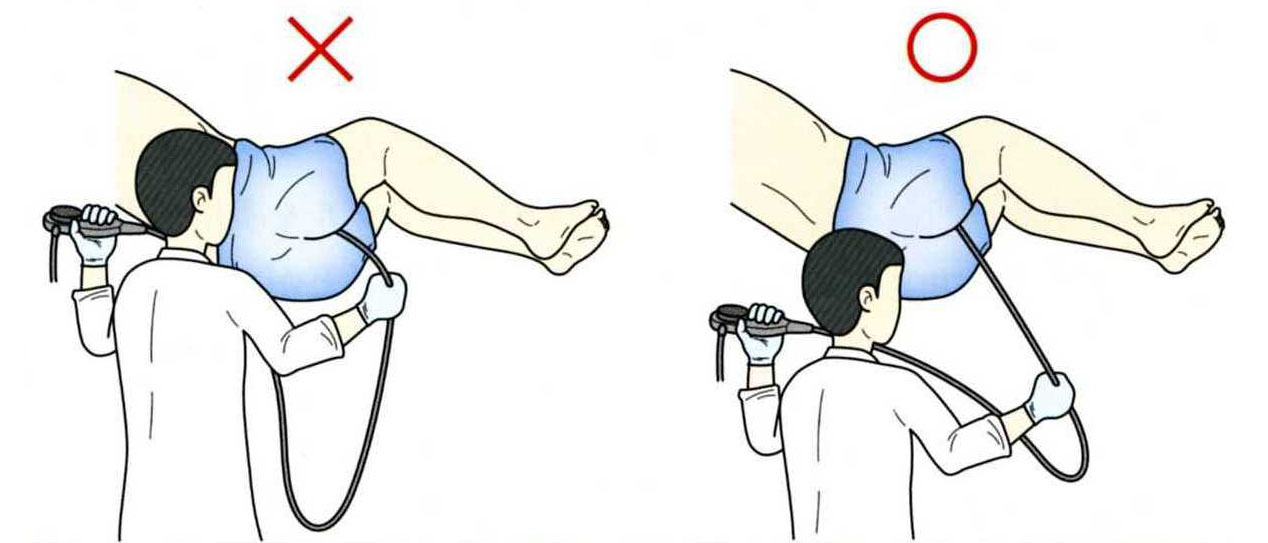
Chart 8-7 There is another reason why the right hand should not be too close to the anus (Chart 8-7). At the start of the intubation, the scope outside of the body is long and if the right hand is too close to the anus, the scope will droop like the left picture in the chart. In this situation, the left hand movement cannot make the rotation of the scope. The rotation with only the left hand is possible only when the right hand is at least 30cm away from the patient. |
Å@
|
MOVIE 8-1 HOW TO HOLD THE SCOPE PUT THE SCOPE ON THE PALM FACING UPWARD FORIZONTALLY AND HOLD THE SCOPE SOFTLY. |
Å@